42 year old male with shortness of breath and pedal edema
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
A 42 year old male who is a labourer by occupation came with the cheif complaints of fever since 15 days back, shortness of breath since 5 days and pedal edema since 5 days.
HOPI :
Patient was apparently asymptomatic 1 and half year back and then he developed fever for 3 days and went to local hospital and was diagnosed Hypertension and was on antihypertensive medication since then.
Then he developed shortness of breath ,pedal edema 1and half year ago and went to local hospital where he was told to have a kidney problem later he visited our hospital for same problem where he was evaluated and he was on conservative management for 1 and half year and later initiated in dialysis since 2 months.
15 days back when patient was sitting in a chair at his house he suddenly felt irritation in his right eye followed by watering and the next day patient has pain in the right eye and sudden loss of vision for which he visited an opthalmologist and eye drops were given
Associated with fever which was high grade , continuous not associated with chills and rigor.
Since 5 days back patient is complaining of shortness of breath which was insidious in onset and gradually progressive grade 3 relieved on taking medications.
he developed pedal edema which is pitting type below the knee.
No history ,cold,cough.
No history of burning micturition,chest pain, palpitations, paroxysmal nocturnal dyspnea,syncopal attacks.
PAST HISTORY:
K/C/O HTN since 1 and half year ona tab telma 40 mg.
CKD since 1 and half year on dialysis 2 months.
N/K/C/O asthma ,TB, epilepsy, Diabetes.
Family history:
Not significant
PERSONAL HISTORY:
Diet : mixed
Appetite : decreased
Urine output: normal
Bowel and bladder movements: regular
Sleep : adequate
Addictions : alcohol occasionally since 20 years during night time but stopped since 1 and half year back.
He studied till 10th class and stoped
He is labour by occupation previously but stopped one and half year back
Married 26 years back
2 childrens female 23 years got married
Male 20 years he is studying
DAILY ROUTINE
Until one and half year ago he worked as labour .
Now he wakes up 8am .he takes his breakfast at 8.30 am and does his daily activities.
He then take lunch at 1pm and dinner at 9pm and goes to sleep at 9.30 pm.
GENERAL EXAMINATION
Patient was conscious, coherent, and cooperative.
Moderately built and moderately nourished.
Pallor : present
Cyanosis: absent
Clubbing: absent
Edema: present
Icterus: absent
Lymphadenopathy: absent





Vitals
Temperature : afebrile
BP: 150/100 mmHg
PR: 100 bpm
RR : 20 cycles/min
SYSTEMIC EXAMINATION:
Cardiovascular system:
Inspection:
Jvp
Apex beat visible
No scars, sinuses, dilated veins
No precordial bulge is seen.
Palpation:
All inspectory findings are confirmed
Trachea is central
No thrills ,heaves or any localised pulsations
Apex beat felt on 5th intercostal space half inch lateral to midclavicular line.
Percussion:
Right and left borders of heart are percussed.
Auscultation
Systolic murmurs heard at mitral , tricuspid, pulmonary,aortic areas.
Murmurs radiated to axillary region.
Respiratory system:
Inspection
Shape of chest is elliptical and bilaterally symmetrical.
Trachea appears to be central
No scars , sinuses, engorged veins.
Movements appears to be equal on both sides.
Palpation:
All inspectory findings are confirmed
Trachea appears to be central
Percussion:
Resonant note is heard
Auscultation :
Normal vesicular breath sounds are heard.
Central nervous system:
No focal neurological deficit.
Abdominal examination
soft and non tender ,no organomegaly
Liver not palpable
Spleen not palpable
Bowel sounds heard.
Provisional diagnosis Heart failure?
INVESTIGATIONS:
Hemogram

HBsAg rapid report negative
HIV 1/2 rapid test : non reactive
Blood Grouping and Rh type B +ve
Random blood sugar level 99mg/dl (100 to 160)
Blood urea : 139mg/dl (12to 42)
Serum creatinine:14.1mg/dl (0.9 to 1.3)
Serum electrolytes


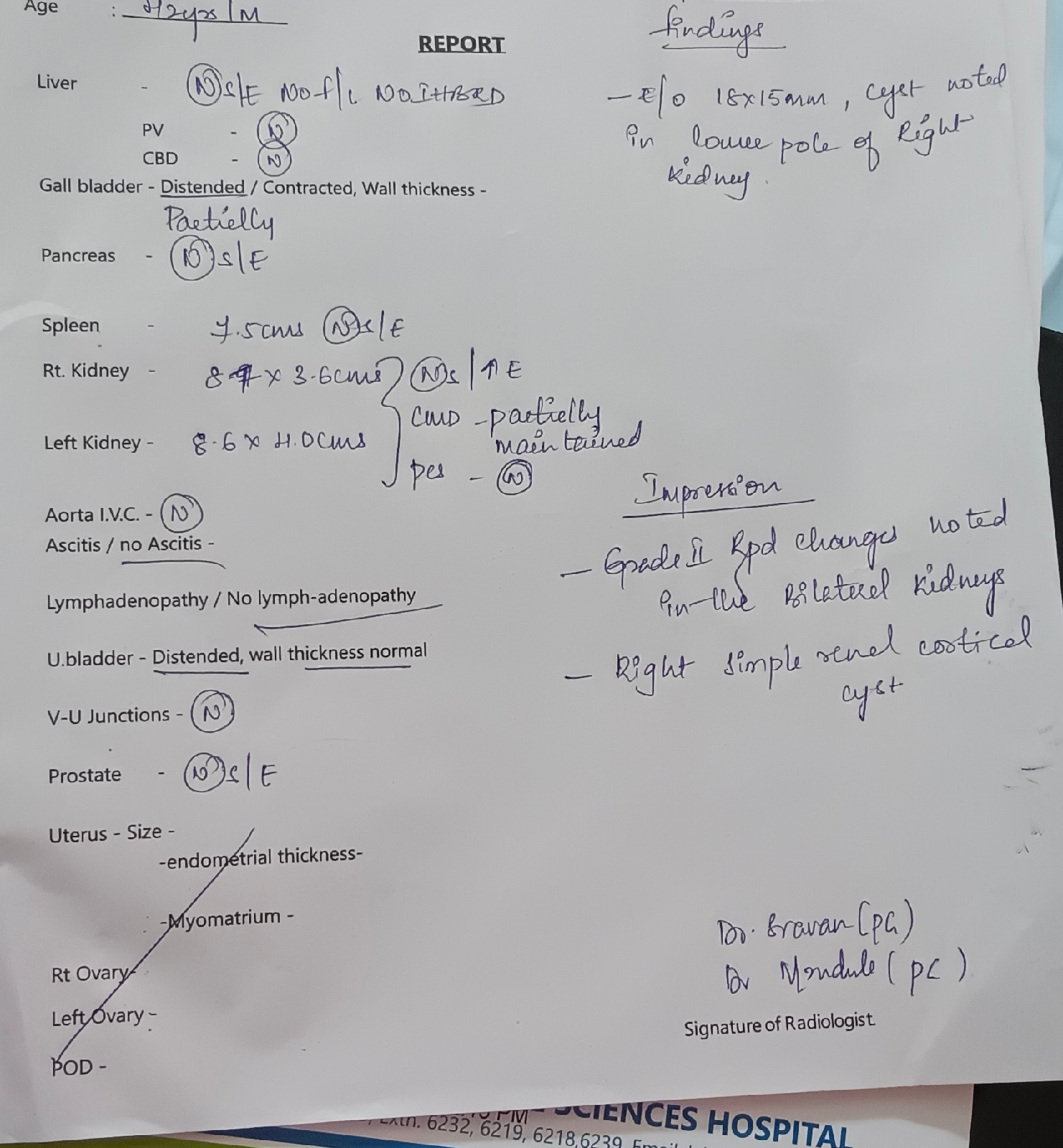
Usg findings :
18*15 mm cyst noted in lower pole of right kidney.
Grade 3 Rpd changes notes in the bilateral kidney
Right simple Renal cortical cyst
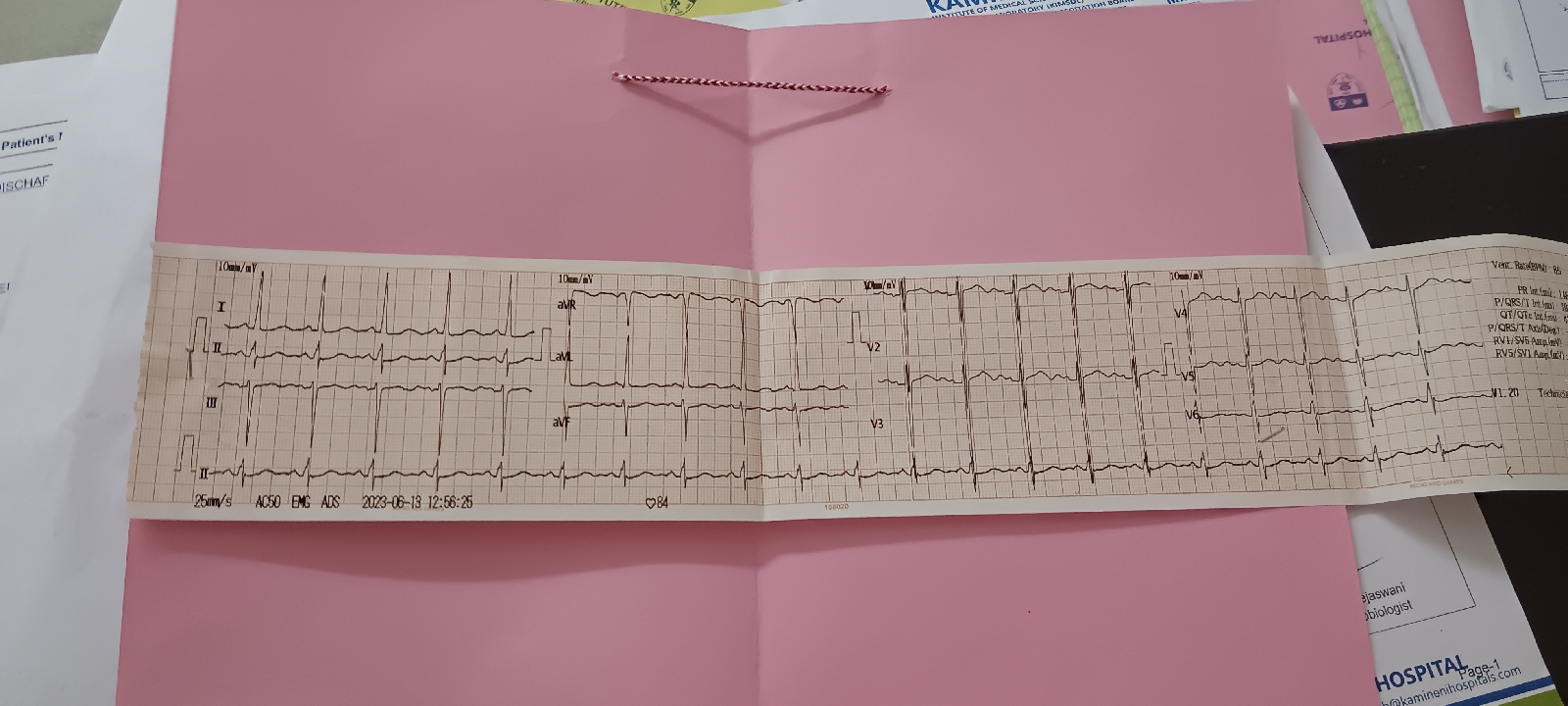
ECG
Final diagnosis:
Heart failure
Anemia of chronic kidney disease
Chronic kidney disease with maintenance hemodialysis
Hypertension
Treatment :
Tab Shelcal
Tab Orofer
Tab Nodosis
Tab Nicardia
Tab Bio D3po

Comments
Post a Comment