A 55 year old with fever and yellowish discoloration
Medical case discussion
July 21,2022
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent
Here we discuss our patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs
This E log book also reflects my patient - centered online learning portfolio and your valuable inputs inthe comment box are welcome.
I have been given this case to solve an attempt to understand the topic of "patient clinical analysis data " to develop my competency in reading and comprehending clinical data including clinical history,clinical findings, investigations and come up with a diagnosis and treatment plan
A 55 year old female from narketpally came with chief complaints of
• Sweating ,generalised weakness, dizziness since 18/7/2022 morning 5.30.
• Fever, yellowish discoloration of urine and eyes since 20 days
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 20 days back , then she developed fever - intermittent (4 or 5 times since 20 days) and evening rise of temperature was seen for which she took paracetamol and it subsided . Fever was not associated with chills and rigors.
She also had yellowish discoloration of eyes and urine since 20 days .
She also complains of burning micturition.
2 weeks back( on 1/7/22) she came to our hospital and was asked to get admitted but due to financial problems their family denied it.
Treatment advised were- tab Udiliv 300mg BD,
MVT OD, Tab Dolo 650mg sos, continue antihypertensive and anti diabetic medications.
And then she took herbal medicines every monday for 2 weeks and stopped anti diabetic and anti hypertensive medications completely since 1 week(when she started taking herbal medications).
Two days back (18/7/22 ) she had difficulty passing urine and then she developed generalised weakness, dizziness and sweating and came to Kims and got admitted.
PAST HISTORY
Known case of diabetes and hypertension since 6 years
Not a known case of asthma, tuberculosis, epilepsy.
PRESENT HISTORY
Daily routine :
She was an agricultural labourer by occupation.
She quit working since 6 years after she was diagnosed with diabetes and hypertension.
Wakes up at 6 AM
Does household work
Breakfast at 9 AM
Watches tv, cooking
Lunch at 1 PM
Sleeps, does some household work
Dinner at 8 PM
Sleeps at 9 PM
PERSONAL HISTORY
Diet: mixed
Appetite: normal
Bowel and bladder movements
Yellowish urine, burning micturition.
Difficulty passing stools
No known food allergies
Sleep: adequate
Addictions : toddy but stopped 6 years ago.
TREATMENT HISTORY
Medication for headache frequently
Using Amlodipine for hypertension
And glimiperide, metformin for diabetes
Since 6 years
IMMUNIZATION HISTORY
Vaccination upto date
Vaccinated for Covid-19
GENERAL EXAMINATION
Patient is conscious, coherent and cooperative.
Well oriented to time place person
Moderately built and moderately nourished
No pallor
Icterus present
No cyanosis
No clubbing
No lymphadenopathy
No edema
Patient is conscious, coherent and cooperative.
Well oriented to time place person
Moderately built and moderately nourished
No pallor
Icterus present
No cyanosis
No clubbing
No lymphadenopathy
No edema
VITALS
PR: 80bpm
RR: 16cpm
TEMP :Afebrile
BP: 140/90mmhg
SP02 :99%
GRBS : 145 mg/dl (19/7/22)
SYSTEMIC EXAMINATION
RS: BAE+, NVBS
CVS : S1 S2 heard, no murmurs
CNS: NFD
PA:
Shape- obese
No tenderness
No free fluid present
Umbilicus- normal
Movements -moves with respiration
No sinuses, distended veins
Scar of hysterectomy 20yrs back
No palpable mass
Liver is palpable
Spleen is not palpable
Bowel sounds heard
No bruits





On 23/7/22


On 1/7/2022












ON 18/7/2022












ON 19/7/2022






On 21/7/22


On 23/7/22



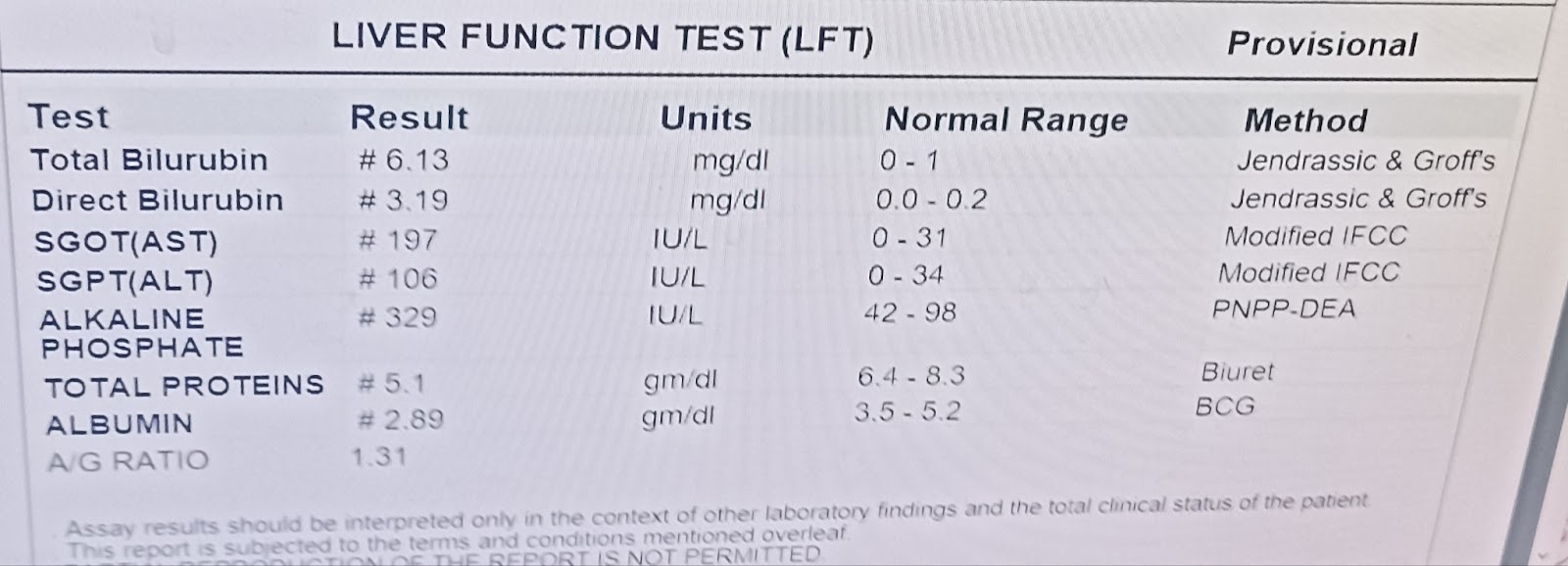


PROVISIONAL DIAGNOSIS
TOXIN INDUCED HEPATITIS
TREATMENT
1. Inj Pantop 40mg OD IV
2. Inj Zofer 4mg IV
3. Inj Neomol 1gm IV
4. Tab PCM 500mg BD
5. Tab Rifagut 550mg
6. Inj Trenexa 500mg IV stat
7. Tab Udiliv 300mg BD
8. Syrup Lactulose
9. Syrup Aristrozyme 25ml TID
10. Protein rich diet
11. Temperature charting ,GRBS monitoring .

Comments